
Everyone says tirzepatide is simply the better drug because it beat semaglutide’s number in the trials. Everyone is wrong, or at least half wrong, and I want to walk through why before I concede the one point where the crowd is actually right.
Last updated: June 2026. Quick housekeeping before I make my case: semaglutide (Wegovy, Ozempic) and tirzepatide (Zepbound, Mounjaro) both cleared the FDA on the strength of large human trials. Neither is a guess. The compounded versions of either drug are mixed by a compounding pharmacy and live in a different regulatory lane than the branded, FDA-approved products. Every figure below traces to a specific trial or label, cited in the numbered references, so you can go check my work. And no, I can’t tell you which drug is right for you. Neither can any article. A clinician who has actually reviewed your history can, and that distinction is going to matter more than you think by the end of this piece.
The argument everyone makes
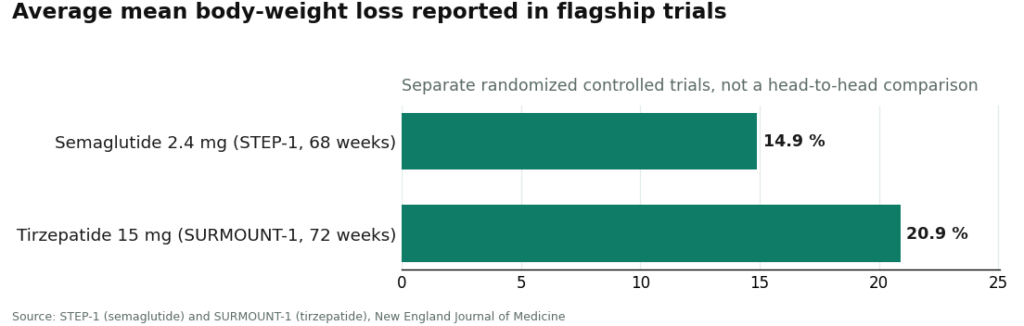
Open any comparison page on this topic and you’ll hit the same table almost immediately: tirzepatide, 20.9% average weight loss at 72 weeks in SURMOUNT-1 [2]. Semaglutide, 14.9% at 68 weeks in STEP-1 [1]. Bigger number wins, conversation over, go get the tirzepatide.
I understand the appeal of that logic. It’s clean. It fits on a chart. And it isn’t fake, that gap is real, drawn from two separate randomized controlled trials published in the New England Journal of Medicine, the gold standard for this kind of evidence. But treating “which number is bigger” as the whole decision is where people go wrong, and I think the reasoning falls apart the moment you look at it closely.
Here’s the evidence against the obvious take
These trials never raced each other. STEP-1 and SURMOUNT-1 studied different groups of people at different times. Nobody flipped a coin and randomized the same population directly between the two drugs. So the 14.9%-versus-20.9% gap tells you the two trial averages differed. It does not tell you what would happen if you personally took one versus the other. Treating it as a precise personal margin is a category error dressed up as data.
The 20.9% figure is a best-case cherry, not the whole story. SURMOUNT-1 actually reported a range of roughly 15.0% to 20.9% mean weight loss across the 5 mg, 10 mg, and 15 mg doses [2]. That top number is the top dose. Lower tirzepatide doses land right in semaglutide’s neighborhood. The clean “20.9 beats 14.9” framing quietly assumes everyone ends up on the highest dose, which is not how titration works for every patient.
Averages erase the individuals who don’t fit them. Both trials are reporting means across hundreds of people. Real bodies scatter widely around a mean. Plenty of people on semaglutide will outlose the tirzepatide average, and plenty of people on tirzepatide will land under the semaglutide average. A population statistic is not a personal forecast, no matter how many headlines treat it like one.
The two drugs share the exact same serious warning, and almost nobody leads with that. This is the part I think gets buried under the percentage race. The FDA-approved labels for both products carry a boxed warning, the most serious kind, for thyroid C-cell tumors, and both contraindicate use in anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [3]. That’s not a minor footnote. It’s identical across both drugs. If that history rules you out of one, it rules you out of the other. Switching brands doesn’t get you around it. Both also carry warnings around pancreatitis and gallbladder disease that a clinician has to monitor for [3]. So before anyone gets to argue about 15% versus 21%, there’s a screening question that has to come first, and the trial table has nothing to say about it.
Side effects, too, run largely in parallel rather than in competition. Both drugs act on gut signaling and slow gastric emptying [4], so both produce the same family of complaints, nausea, vomiting, diarrhea, constipation, worst early on and during dose increases, which is exactly why both are titrated up slowly. If nausea from one mechanism wrecks you, that’s a real data point for your clinician to weigh, though it doesn’t automatically predict how you’ll do on the other.
The honest concession
Now, the part where I have to admit the crowd isn’t entirely wrong. Tirzepatide really does activate two receptor pathways instead of one, GLP-1 like semaglutide, plus GIP, a second gut hormone involved in insulin and metabolism [4]. That dual mechanism is the leading explanation for why its trial averages ran higher, and the size of that effect, a mean of 20.9% at the top dose against 3.1% on placebo [2], is a genuinely larger number than semaglutide’s 14.9% against 2.4% on placebo [1]. I’m not going to pretend that gap doesn’t exist or doesn’t matter. If you’re purely optimizing for the single biggest average effect size reported in a phase-3 trial, tirzepatide is the honest answer to that specific, narrow question.
But “biggest average in a trial” and “right drug for you” are different questions, and conflating them is exactly the mistake I opened this piece attacking.
See also: The Rise of Data Literacy: Why Statistical Competency is Non-Negotiable in Modern US Careers
So what actually decides it
Once you set the percentage race aside as the sole criterion, several other factors get to speak, and any one of them can flip the choice:
- What you can actually tolerate. The drug you can stay on without being sick every week beats the drug with the better trial average that you quit taking after six weeks.
- The depth of the evidence base. Semaglutide has been studied across weight, diabetes, and cardiovascular outcomes for longer, and depending on your health picture that breadth can matter more than a single weight-loss column.
- How your specific body responds. People respond differently to different molecules, and that only becomes clear once you’re actually on one.
- What you can access and afford. This shifts by person and by month, and it’s a legitimate part of the real-world decision even though no trial measures it.
- Your own history, read by someone qualified to read it. Other conditions, other medications, other goals, all of it feeds into which drug is the smarter starting point, and that’s a clinical judgment, not a spreadsheet formula.
The honest summary: the bigger number makes tirzepatide a strong option. It does not make it the automatic right answer for every person reading this. Semaglutide is still an excellent, proven drug, and for plenty of people it’s the better one.
The actual decision framework
So don’t decide from the table. Bring the table to someone who can put it next to your chart. The trial numbers should inform that conversation, not substitute for it. Because both drugs carry the identical thyroid contraindication [3], a screen isn’t optional for either one, and running that screen is a clinician’s job, not a website’s.
This is also why I think the where matters as much as the which. Either molecule, chosen well, still requires someone checking you against the label, walking you up the dose ladder slowly, following up over time, and a licensed pharmacy actually filling a consistent product. None of that exists when a site hands over a vial with no prescription required, the kind of operation that will never ask you about medullary thyroid carcinoma in your family because asking would slow down the checkout. FormBlends is one outfit built the other way: a clinician evaluation, a screen against the label, a prescription written only when it’s appropriate, a licensed pharmacy dispensing it, and more than one GLP-1 actually on offer instead of a single locked-in product. I’m naming it to show what the supervised version of this looks like in practice, not to declare a winner between two medications that both deserve real consideration.
The semaglutide-versus-tirzepatide question is worth taking seriously. It just doesn’t get answered by whichever number is bigger on a comparison table. It gets answered in a room with someone who’s actually looked at your chart.
Quick summary, stripped of spin
- Mechanism: semaglutide hits one receptor pathway (GLP-1); tirzepatide hits two (GLP-1 and GIP) [4].
- Average weight loss: about 14.9% for semaglutide in STEP-1 [1], about 20.9% at the top dose for tirzepatide in SURMOUNT-1 [2]. Separate trials, not a head-to-head, both real.
- Side effects: both gastrointestinal-heavy with slow titration; both carry the identical thyroid C-cell tumor boxed warning and MTC/MEN 2 contraindication [3].
- The tiebreaker isn’t the percentage. It’s tolerability, your broader health history, how your body actually responds, access, and a clinician’s read on your case.
What is semaglutide?
Semaglutide is a prescription medication that copies a hormone your gut already makes, called GLP-1. It got its first approval for type 2 diabetes under the name Ozempic, then a later approval at a higher dose for weight management under the name Wegovy. Same molecule, different dose, different label.
How does semaglutide actually work in the body?
It latches onto GLP-1 receptors in the pancreas, brain, and gut. That slows how fast your stomach empties and tells your brain you’re full sooner than usual. It also nudges the pancreas to release more insulin after meals and turns down glucagon, a hormone that pushes blood sugar up. The appetite effect is the reason it became the center of the weight-loss conversation in the first place.
Does it actually work for weight loss, or is that overstated?
It works, and the evidence isn’t ambiguous on that point. The trials behind Wegovy’s approval showed average weight reductions around 15% over roughly 68 weeks, though individual results spread out quite a bit around that average. It works best paired with real changes to eating and activity, and weight tends to come back if you stop taking it, which is worth knowing going in rather than finding out later.
Is semaglutide safe? What should worry me?
It has a large, well-documented safety record from trials and years of real-world use, but “well-documented” isn’t the same as “risk-free.” Nausea, vomiting, and constipation are the common complaints, especially in the early weeks. On the rarer, more serious end sit pancreatitis and, based on animal data, a possible thyroid-tumor risk, which is why the label carries a boxed warning. Getting it through a physician-supervised channel, a licensed compounding pharmacy such as FormBlends, keeps the screening and dose titration part of the deal instead of leaving it out.
References
- STEP-1 trial: once-weekly semaglutide 2.4 mg produced about 14.9% mean body-weight loss at 68 weeks versus about 2.4% on placebo. Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, 2021. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- SURMOUNT-1 trial: tirzepatide produced mean weight loss of roughly 15.0% to 20.9% across the 5, 10, and 15 mg doses at 72 weeks, with about 20.9% at the 15 mg dose versus about 3.1% on placebo. Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, 2022. PMID 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/
- FDA-approved labels for semaglutide (Wegovy) and tirzepatide both carry a boxed warning for thyroid C-cell tumors and contraindicate use with a personal or family history of medullary thyroid carcinoma (MTC) or MEN 2, with additional warnings including pancreatitis and gallbladder disease. Wegovy label, Novo Nordisk, DailyMed (FDA label).
- GLP-1 receptor agonist mechanism (the pathway both drugs share): glucose-dependent insulin secretion, slowed gastric emptying, appetite reduction; tirzepatide adds GIP-receptor activity. Collins L, Costello RA. “Glucagon-Like Peptide-1 Receptor Agonists.” StatPearls, NCBI Bookshelf.
.